The Forum is Open! April 11, 2008
Posted by tomography in Nuclear Medicine, Picture of the week, Radiology, Rare Cases.add a comment
![]() I am proud to let you know that our Forum is now officially open! With the full support of the Debrecen Medical and Health Science Center Radiology and Nuclear Medicine Departments we have set off to collect interesting, rare clinical cases. Submissions are also accepted continuously! We are inviting all radiologist, nuclear medicine specialists, technicians from all over the world to take part in this great initiative. Contributors will be awarded in some way, and some submissions may be recommended for publishing with consent of submitter.
I am proud to let you know that our Forum is now officially open! With the full support of the Debrecen Medical and Health Science Center Radiology and Nuclear Medicine Departments we have set off to collect interesting, rare clinical cases. Submissions are also accepted continuously! We are inviting all radiologist, nuclear medicine specialists, technicians from all over the world to take part in this great initiative. Contributors will be awarded in some way, and some submissions may be recommended for publishing with consent of submitter.
Terms and Conditions to this Forum:
- All readers of TomographyBlog.com may take part in this forum either by submitting new cases, or by sending us their solutions.
- Please elaborate on the solutions by writing to the “comments section” of a page.
- You are welcome to submit cases from your own clinical practice and submission is not limited to Radiology nor Nuclear Medicine.
- Submissions are accepted via email: tomographynm (at) gmail.com
- Images and cases that appear here may be used only for educational purposes and by clearly indicating TomographyBlog.com as Source.
On the Forum page you will also find our successful Picture of The Week series with solutions. I encourage you to sign up to our RSS Feed to receive all new cases on time. Click the RSS logo to sign up:

Solution to picture of the week #8, and this week’s image November 24, 2007
Posted by tomography in Picture of the week, Radiology.Tags: CT, Ductus Botalli, fetal circulation, Trichophagia
2 comments

Ductus botalli is one of three vital shunts in the fetal circulation. The other two are the foramen ovale, and the ductus venosus. After birth, smooth muscle cells in the ductus Botalli react to falling levels of prostaglandin by constriction therefore reducing the flow of blood in the vessel. It is usually completely closed by the fourth up to the tenth day after birth, and it is reduced to what is known by the name of ligamentum arteriosum.
Failure of closure (patent ductus arteriosus) results in a left-to-right shunt in the newborn’s circulation. This in turn allows oxygen rich and poor blood to mix, and may also lead to pulmonary hypertension, heart failure, and arrhythmia. Conservative treatment includes non-steroid anti-inflammatory drugs, for instance indomethacin or ibuprofen. If conservative treatment fails, surgical correction isinevitable.
———————————————————————————————
You will never guess what this week’s image is, or will You?! Give it a try:

Solution to Picture of the week #7, and this week’s image. November 13, 2007
Posted by tomography in Picture of the week.add a comment

Pneumothorax is very painful and potentially life threatening. It may occur on the bases of several underlying diseases, but mostly due to trauma (e.g. broken ribs), rupture of an emphysematosus bulla, trans-thoracic fine needle biopsy, or as a result of artificial respiration. It is life threatening because it acutely diminishes lung capacity and causes the dislocation of the greater vessels. Most patients complain of a sharp, sudden pain and may become cyanotic very quickly. Dislocation of the mediastinum may result in insufficient cardiac output, and if blood circulation does not match demand, the patient may collapse or even die.
End here is this week’s image:

Starting next week, you will find 5 pictures per week under the “Quiz” page on the main menu. Please, email us your answers; do not write them on the comment section! This nuclear medicine quiz is going to last for 5 weeks, and it is open to everyone, but only students attending the University of Debrecen can earn extra points on their final exam. Good luck!
Solution to Picture of the week #6, and this week’s image. October 23, 2007
Posted by tomography in Megaureter, Nuclear Medicine, Picture of the week.Tags: Megaureter, renogram dynamic renal scan, ureter peristalsis
3 comments
 Last week’s image was taken during a dynamic renal scan, and the image obtained was a so called renogram. During this technique metastable 99-Technetium labeled mercapto-acetyl-triglicine (MAG-3) is administered intravenously to the patient, and (s)he is placed under a gamma camera. The tracer, MAG-3, travels through the bloodstream, and (if the renal perfusion is adequate) it is excreted by the kidneys. As the traces travels, it emits gamma rays, that are recorded by the gamma camera. On average, data is collected for ten seconds for an image, during which, individual gamma photons are allowed to “stain” the diagnostic picture. Generally, the longer the tracer “stays” in one place (due to an obstruction for example), the more gamma photons will contribute to the stain for the given location. So if the configuration of the kidney-ureter-bladder system is physiological, it will have more staining in the pelvis of the kidney, and the bladder, but the ureter will not show, given that the speed of each bolus is normal, which is about 15-20 mm/second.
Last week’s image was taken during a dynamic renal scan, and the image obtained was a so called renogram. During this technique metastable 99-Technetium labeled mercapto-acetyl-triglicine (MAG-3) is administered intravenously to the patient, and (s)he is placed under a gamma camera. The tracer, MAG-3, travels through the bloodstream, and (if the renal perfusion is adequate) it is excreted by the kidneys. As the traces travels, it emits gamma rays, that are recorded by the gamma camera. On average, data is collected for ten seconds for an image, during which, individual gamma photons are allowed to “stain” the diagnostic picture. Generally, the longer the tracer “stays” in one place (due to an obstruction for example), the more gamma photons will contribute to the stain for the given location. So if the configuration of the kidney-ureter-bladder system is physiological, it will have more staining in the pelvis of the kidney, and the bladder, but the ureter will not show, given that the speed of each bolus is normal, which is about 15-20 mm/second.
The correct answer was, indeed, megaureter as all of you correctly suggested. You may read a very detailed review on the subject via this link, or you may wait until I post my next topic titled “How to detect a megaureter?”
And now, here is this week’s image. Good luck, and see you back here next time!

Solution to Picture of the week #5, and this week’s image. October 16, 2007
Posted by tomography in Nuclear Medicine, Picture of the week.4 comments
You guys were right, the answer to last week’s image was bullous lung disease due to emphysema. The x-ray shows wide intercostal spaces and the fine outline of the bullas. The CT scan comfirms the presence of the bullas, and the absence of lung tissue and bloodvessels in them. Here is the link to this image, where you can read more about this disease.
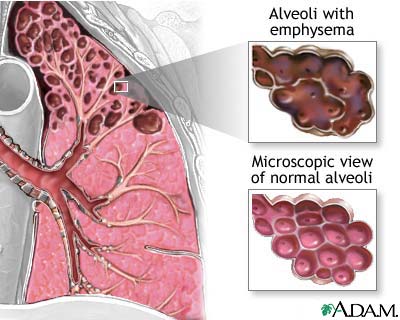
Also check out this wonderful picture on the different types of emphysema. This would have made it so much easier for us to understand them when we were cramming the list, don’t you think so? Aah, the good times we shared in Pathology! 🙂

And here is this week’s image. The questions:
- What kind of technique was used to obtain it?
- What is not physiological in this case?

Stress and Test October 16, 2007
Posted by tomography in Nuclear Medicine, Picture of the week, SPECT.6 comments
 The stress test shows if your heart receives enough blood from its own arteries to work harder, safely. Taking the stress test also helps your doctor know what type of exercise and how much is right for you.
The stress test shows if your heart receives enough blood from its own arteries to work harder, safely. Taking the stress test also helps your doctor know what type of exercise and how much is right for you.
The role of nuclear cardiology
The resting heart muscle’s blood supply needs are usually well met even in the presence of blocked arteries. When the heart is stressed either by exercise or chemicals, the demand for blood increases. The blood flow through the blocked arteries – while adequate at rest – may not be able to keep up with the demands of a stressed heart. This can show up on the pictures of the heart taken after stress. This is the principle behind all the stress tests. The word stress test is used for any means used to increase heart muscle’s demand for blood. This can be done by exercise or by chemical means.
The patient either walks on a treadmill, or is given iv. (intravenous) medication which simulates exercise, while connected to an ECG machine, used to record a 12-lead ECG. The level of exercise is increased by 3 minute stages, of progressively increased grade (incline) and speed. The patient’s symptoms, and blood pressure (BP) response are repeatedly checked.
However, some patients cannot exercise adequately. Patients with lung disease, arthritis, or disease in the leg vessels may not be able to walk. Patients with some medical conditions should not walk on the treadmill. For these patients the doctor can use a drug to affect the blood supply to the heart and simulate the effects of exercise.
It is done to identify the cause of chest pain or chest discomfort which can occur with blockages in blood flow to the heart, to monitor heart function in people with known heart disease, and to determine the response to medications or after angioplasty or bypass surgery.
If radioactive isotopes are also used (commonly, Technetium Tc99m Sestamabi and rarely, Thallium-201), then it is usually called a Nuclear Stress Test (NST).
The most commonly used NST is the Dobutamine Nuclear Stress Test (Cardiolite). (There are four types of cardiolite stress test. Excersize, Persantine, Adenosine and Dobutamine stress test.)
It is similar to excersize stress test except for the fact that a medicine called Dobutamine is used to stress the heart. During this test, Dobutamine is infused at a gradually increasing rate to increase the heart rate to a desired level. This drug has the effect of increasing the force of contraction of the heart, the heart rate and blood pressure. This stresses the heart muscle, which simulates exercise.
“Cardiolite is a short-lived, radioactive element that is absorbed by the heart muscle and allows your heart to be seen by the camera. Cardiolite images allow the physician to indirectly look at the blood flow to your heart.”
Areas that do not have adequate blood supply pick up the tracer very slowly or not at all.
Take a look at one of the “picture of the week”s.
Cardiolite is injected while you are at rest and while your heart is under stress. Rest and stress images are taken to allow doctors to compare how much blood flows through the heart muscle during stress and at rest.
(Most patients experience no side effects.)
“Persantine is a coronary vasodilator that is used as a diagnostic agent in nuclear stress testing. Persantine works by increasing the blood vessel circumference of the coronary arteries (arteries that feed the heart) in order to increase blood flow to the heart.”
Adenosine is an antiarrhytmic agent, works as a vasodilatator, similar to Persantine. Side effects include: chest pain/pressure, headache, nausea, dizziness, shortness of breath. Some patients experience a burning or stinging sensation at their IV site because Persantine is more acidic than your blood. Persantine is contraindicated in patients who have a hypersensitivity to this drug. If needed, the antidote Aminophylline is given to the patient.
Solution to Picture of the week #3, and this week’s image. October 2, 2007
Posted by tomography in Picture of the week, Uncategorized.1 comment so far
Take a look at the following image, that will help you better visualize the way SPECT images are taken. Therefor, if you go back to last week’s image, which as zslog pointed out was taken after the so-called dobutamine stress test, you may easily identify the parts with poor perfusion. (Scroll down for the solution to last week’s image).

Solution to image of the week # 3:
- From the HLA – horizontal long axis view – you can tell, that the septum has perfusion defect, and
- From the SA – short axis view – and the VLA – vertical long axis view – you can tell that the apex of the heart is hypo-oxygenated.
And here is this week’s image:

- What kind of image is this?
- Identify 3 abnormalities on it.
- What could have caused this trauma?
Picture of the week #3 September 25, 2007
Posted by tomography in Picture of the week, Uncategorized.2 comments
Thoracic pain is a quite common and freightening symptom that can be caused by various reasons. Based on this SPECT image, what is the origin of pain in this case?



 Flock
Flock